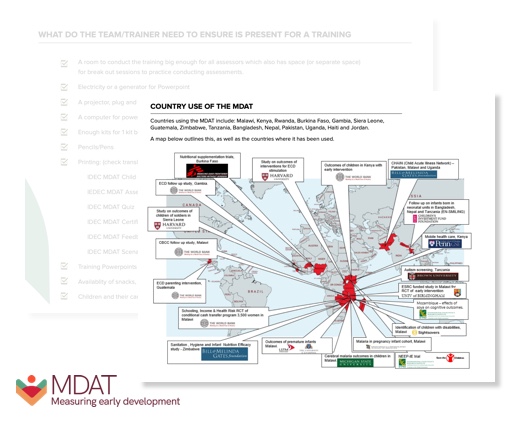
Poor child development affects over half of all children globallyleading to poor future human capital. Goals now set by United Nations strive to address this (SDG 4.2.1) but agencies are hindered by available tools to measure change. Most tools are costly, culturally inappropriate and complex. Malawi Developmental Assessment Tool (MDAT) is currently used in >25 countries enabling agencies (World Bank, Save the Children, Medicins Sans Frontiers) to measure child development, promoting the investment of > $90 million and benefitting > 400,000 children. MDAT methodology underpins new ECD measurement tools for WHO, UNICEF, and World Bank for future tracking of SDG 4.2.1
Lack of a Suitable Tool to Measure Child Development in LMIC Settings:
Gladstone’s early clinical research in Malawi identified worrying developmental delays in children sick with HIV, malaria and malnutrition. Improved medical care globally meant that more children than ever were surviving but suffering developmental delays and associated disorders. The major problem, Gladstone realised, was the lack of a robustly validated tool to measure early child development (ECD) in a simple, cheap, culturally specific way for young children (0-5 years). Such an assessment tool is essential for the evaluation of children and their response to interventions in an African context. Existing tools were complex, primarily American (not culturally relevant), and prohibitively expensive (approximately GBP 1,500/ kit). It was thus impossible to measure ECD or quantify improvement following clinical or public health interventions.
Our multidisciplinary University of Liverpool team, Gladstone (Neurodevelopmental Paediatrics), Smyth (Paediatrics) and Lancaster (Biostatistics), conducted preliminary studies detailing difficulties using Western tools [3.1], and used qualitative studies to unravel the conceptualisation of child development in African contexts. We then iteratively developed Malawi Developmental Assessment Tool (MDAT), a valid tool relevant to motor, language and social development of young children in Malawi and elsewhere in Africa [3.2]. We then refined and robustly tested MDAT using detailed psychometric techniques creating population-based age-bands for developmental milestones for 1,446 children from 0-6 years (PLoS Med 2010) [3.3]. MDAT has a simple-to-use scoring system [3.3], is sensitive to differences between children with different medical conditions and is predictive of later school achievement [3.4][3.5]. MDAT has now been validated in over 200 studies, many in high impact journals.
MDAT use in major intervention programme evaluations leading to further investment:
The NEEP-IE study (Save the Children) in Malawi, (with Liverpool involvement), used MDAT to evaluate impacts of childcare centre-based integrated nutritional and agricultural interventions on diet, nutrition and development in young Malawian children [3.6]. This work, alongside other studies in Malawi (including PECD study, an evaluation of children’s development with improved access to Community-Based Child Care Centres, independent of UoL MDAT team), utilised the MDAT and the evidence has led to further investment and significant impact. Similar studies in the Gambia (World Bank and without UoL MDAT team involvement) also used MDAT to evaluate children’s development in hundreds of Community-Based Child Care Centres, also leading to a scale-up of investment.
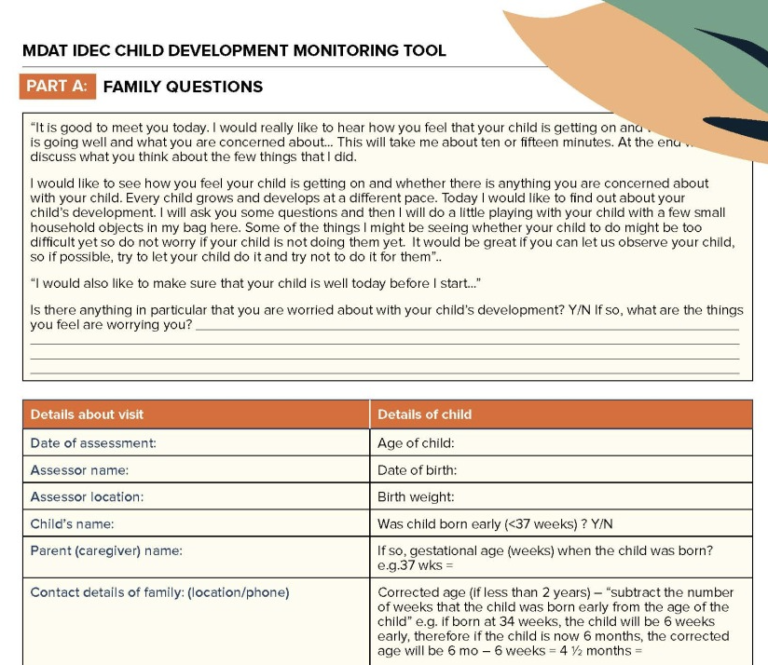
Adaptions of the MDAT to produce separate evaluation tools, widening scope and application are ongoing. These include the development of a mobile app for use in Kenya, Haiti and Uganda (the UNICEF IDEC project). The MDAT app incorporates the MDAT red flag system to support decisions on individual child referrals and over 150 community health workers are receiving training to use the tool. Also, in Uganda and Malawi, the MDAT is used as a screening tool for new interventions to support mothers of children with disabilities. This has already provided clear evidence as to the prevalence of child disability within these settings, identifying where improved services and support are required.
References
[3.1 ] Gladstone, M., Lancaster, G., Jones, A., Maleta, K., Mtitimila, E., Ashorn, P. & Smyth, R. L. 2008. Can Western developmental screening tools be modified for use in a rural Malawian setting? Archives of Diseases of Childhood, 93, 23-29.
[3.2] Gladstone, M., Lancaster, G., Umar, E., Nyirenda, M., Kayira, E., Van Den Broek, N. & Smyth, R. L. 2010a. Perspectives of normal child development in rural Malawi – a qualitative analysis to create a more culturally appropriate developmental assessment tool. Child Care Health Dev, 36, 346-53.doi: 10.1111/j.1365-2214.2009.01008.x
[3.3] Cheung, Y. B., Gladstone, M., Maleta K., Duan, X. & Ashorn, P. 2008. Comparison of four statistical approaches to score child development: a study of Malawian children. Trop Med Int Health, 13, 987-93.doi: https://doi.org/10.1111/j.1365-3156.2008.02104.x
[3.4] Gladstone, M., Lancaster, G. A., Umar, E., Nyirenda, M., Kayira, E., Van Den Broek, N. R. & Smyth, R. L. 2010b. The Malawi Developmental Assessment Tool (MDAT): the creation, validation, and reliability of a tool to assess child development in rural African settings. PLoS Med, 7, e1000273. doi: 10.1371/journal.pmed.1000273
[3.5] Gladstone, M, White S, Kafulafula G, Neilson JP, Van den Broek N. Post-neonatal mortality, morbidity, and developmental outcome after ultrasound-dated preterm birth in rural Malawi: a community-based cohort study, PLoS Medicine, 2011 Nov;8(11):
[3.6] Gelli, A., A. Margolies, M. Santacroce, K. Sproule, S. Theis, N. Roschnik, A. Twalibu, G. Chidalengwa, A. Cooper, T. Moorhead, M. Gladstone, P. Kariger, and M. Kutundu. 2017. ‘Improving child nutrition and development through community-based childcare centres in Malawi – The NEEP-IE study: study protocol for a randomised controlled trial’, Trials, doi: 10.1186/s13063-017-2003-7